If untreated, aneurysms can rupture, leading to life-threatening bleeding. While brain aneurysms are common, this article focuses on aneurysms occurring elsewhere in the body. Vascular surgeons treat all aneurysms except for those found within the heart or the brain (which are treated by cardiothoracic surgeons or neurosurgeons / neuro-interventional radiologists)
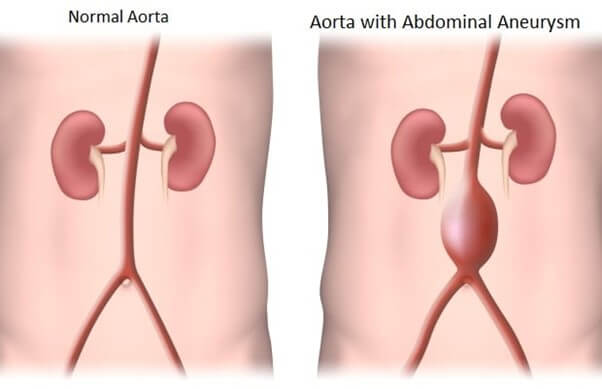
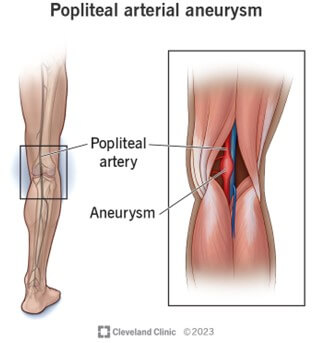
Aneurysms can develop in several vital arteries in the body, including:
Visceral aneurysms
The decision to intervene surgically is based on the size of the aneurysm and the risk of rupture. Standard size criteria include:
Aneurysms are often asymptomatic until they grow large or rupture, but when symptoms do occur, they vary depending on the aneurysm’s location:
Lifestyle modifications, such as quitting smoking, managing blood pressure and cholesterol, and maintaining a healthy weight, are advantageous for slowing aneurysm growth. Patients with aneurysms should be regularly monitored with imaging, and any rapid growth requires prompt medical attention. Studies are being conducted using doxycycline and metformin to reduce aneurysm growth, but this is not yet prescribed or common practice among vascular surgeons at this stage.
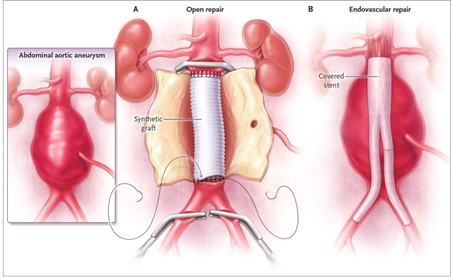
Treatment options vary depending on the size, location, and growth rate of the aneurysm:
Keeping an eye on the size of an aneurysm is essential. All aneurysms will grow, but some may not become large enough to be a problem until you are over 100! You will need someone to monitor its size and growth trajectory. Medicine can help modify risk factors for aneurysm progression.
The choice between open and endovascular repair depends on the patient’s health, the aneurysm’s location and size, and the risks associated with surgery.
The most common discussion to be had involves deciding whether an abdominal aortic aneurysm should be fixed with open surgical repair (big cut) or minimally invasive stent grafting (keyhole surgery).
Pro of minimally invasive
Cons of minimally invasive
Pro of open surgical repair
Cons of open surgical repair