It can severely affect someone’s quality of life. It can be challenging to diagnose, as there are lots of people who have varicose veins in their pelvis who have no symptoms; similarly, some patients have debilitating symptoms.
There is a long list of symptoms, which vary from patient to patient. It is worth noting how many of these symptoms can be caused by other conditions.
Heavy or painful periods or pelvic pain can also be caused by adenomyosis, endometriosis, ovarian cysts, pelvic inflammatory disease, uterine fibroids
Lower back pain and leg pain have a long list of musculoskeletal causes. It could be a muscular injury, ligamentous injury, a bony injury, a protruding disc and many more causes.
Urinary frequency and painful urination can also be caused commonly in women by urinary tract infections.
Other conditions that can cause pelvic pain:
Key message for patients to understand
The key critical concept from reading this article is that many women develop congested pelvic veins and do not have symptoms. Those with symptoms may think the pain is from their veins, but it could be one or multiple other conditions. The safest approach is to rule out all other causes. Intervention on pelvic varicose veins is reserved for patients with severe symptoms when no other cause can be found, provided the symptoms are severe enough to necessitate surgery.
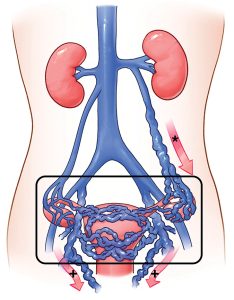
Result of pregnancy and associated hormones – The most common presenting age group would be pre-menopausal women after they have given birth. Hormones related to pregnancy relax the veins, combined with the increased blood volume and pressure of the gravid uterus, which can overwhelm and dilate the pelvic veins, causing the valve leaflets to no longer function as intended. They are unable to restore their function after the blood volume, hormones, and uterus return to normal, leaving the pelvis in a state of permanent venous hypertension. Women who have had multiple children tend to have the highest incidence of pelvic congestion syndrome.
Result of compression of a central outflow vein higher up: Imagine the Princess motorway has had a traffic accident, and cars are backed up for kilometres. The vehicles (blood cells) cannot quickly get to Sydney from Wollongong. Instead, they have to take inland roads and side streets, which quickly get overwhelmed, as the smaller roads can’t cope with the volume of traffic that typically drives from Wollongong to Sydney. When a central vein gets compressed or squashed, something similar happens. The blood can’t pass through the narrowing properly. Hence, the pressure below the compression increases significantly and directs blood through other outflow channels (other smaller veins that eventually lead to the heart but aren’t used to coping with such a large amount of blood).
Overall, this leads to the three causes of pelvic congestion. Two are compression-related, and one is related to changes in pelvic drainage after pregnancy.
Known medically as May-Thurner syndrome. The common iliac vein (main vein that drains the leg and pelvis gets squashed between an artery of the leg and the vertebral column. If this is present, it is something you are born with that can take years to reveal itself as a problem.

Also known as Nut-Cracker syndrome, the vein gets squashed between the large artery of the abdomen and the large artery to the intestines
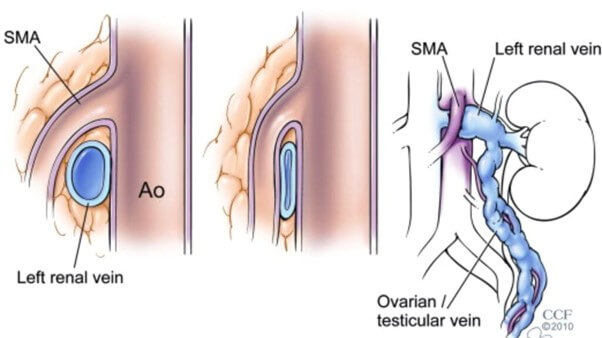
The third cause of pelvic congestion syndrome is a poorly functioning gonadal vein – ovarian vein in women and testicular vein in men. If there is a compressive issue, such as May-Thurner syndrome or Nut-Cracker syndrome, the left ovarian or testicular vein can become engorged. It then eventually become varicose and result in a back-log of pressure in the pelvis and e a cause of pelvic congestion syndrome. Sometimes, women after pregnancy can have an incompetent ovarian vein without any compressive lesion, and the hormones, large pregnant uterus and increased blood volume from pregnancy are enough to damage the ovarian vein, leading to its issues post-delivery.