Spider veins are medically known as telangiectasias. They are small veins that live within the skin and can be red, purple or blue. They often occur in the legs and on the face. They are considered an early form of varicose vein and are typically 0.5-1mm in diameter
Reticular veins often occur along with spider veins and are the ‘feeders’ to the spider veins. They are larger, 1-3mm in diameter, usually blue and live in a layer of the skin deeper than the spider veins.
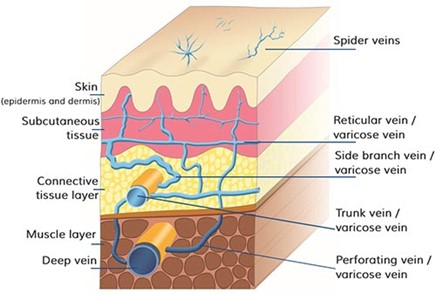
Spider veins and reticular veins are a form of venous insufficiency. This means that the valves within the veins are not working properly.
Spider veins, seen on the skin, are too small to cause very severe symptoms on their own, as the amount of pressure which can build up within such a small vessel is minimal.
It is very common to have venous insufficiency of larger veins that live beneath the skin, which are often the cause of symptoms as well as the cause of the spider veins. It is the larger veins tha which cause most of the problems and should be treated first, as fixing these will often get rid of spider veins. As a patient, you should see a vascular specialist who understands what causes the spider veins, rather than simply seeking out treatment of the spider veins without addressing underlying venous incompetence, as the spider veins will return very quickly if the underlying problem is not addressed.
Spider veins when they occur in isolation are primarily a cosmetic concern, provided your leg has undergone a venous insufficiency ultraosund to confirm that there are no truncal veins that are refluxing and there are no larger veins which are incompetent.

Getting rid of spider veins on the legs is entirely possible. It just requires a stepwise approach and an understanding of their underlying pathophysiology.
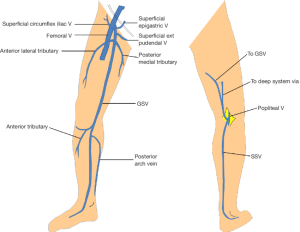
First and foremost, before spider veins are treated, any underlying venous insufficiency of larger truncal veins or varicose veins must be undertaken. Below is a picture demonstrating the superficial truncal veins which often exist as the underlying cause of spider veins
In order to explore treatment options for truncal venous incompetence, visit the section on varicose veins
The two treatment options for spider veins and reticular veins include:
The best treatment depends on the location of the veins, the size of the veins and the number of veins.
Sclerotherapy is the gold standard for treating lower limb reticular veins and spider veins. It involves injecting medicine (sclerosant) which kills veins. If it is done into larger varicose veins, it is often done using an ultrasound (as these structures are deeper and not always felt using your fingers). If it is done on the small reticular or spider veins, this is known as micro sclerotherapy, and often a special light is used to help visualise the feeding vessels to the spider vein.
The injected medicine is passed through a very fine needle, which destroys the wall of the vein. The vein immediately ‘dies’ and when the blood cells are pushed out of the vein, the vein can be seen to disappear.
The main downside is the number of injections required. Larger varicose veins need higher volumes of sclerosant, and only so much sclerosant can be safely used in one sitting. Patients will often require multiple rounds of sclerotherapy to treat a leg full of varicose veins. Spider veins require less volume, so more can be treated in one sitting, but it is time-consuming and painful to have up to thirty injections.
Redness and bruising are common after injection of veins. The redness is from inflammation of the vein that occurs as the body attacks the dead vessel and begins to reabsorb the cells. It typically comes on after 48 hours of the injections.
After sclerotherapy, some people notice a dark or brownish discolouration on their skin where the veins are treated. This happens because a little bit of blood can leak from the treated veins and leave behind a pigment, similar to a bruise turning brown as it heals. Over time, this usually fades, but it can take a few months. In rare cases, it may take longer.
This happens to about 1 in 10 to 3 in 10 people who have sclerotherapy, and while it’s more common in people with darker skin, it can happen to anyone.
To help prevent this, we:
Telangiectatic matting –some people may notice new, tiny red veins or a fine web of blood vessels around the treated area. This happens because the treatment can cause a small amount of inflammation, or the blood flow in the skin may change a little as the treated veins close. These new veins usually fade over time but can last anywhere from a few months to a year. Telangiectatic matting happens in about 1 to 3 out of every 10 people who have sclerotherapy. It’s more common in people who already have a lot of small veins or who are on hormone therapy, like birth control pills.
To help prevent this, we:
As mentioned previously, larger varicose vein systems should be treated first. This starts with an ultrasound assessment of the saphenous veins and deep veins. Once the varicose veins are treated, we move to smaller reticular veins, then spider veins.

Lasers have a wide range of cosmetic applications. Lasers, when targeted at the skin surface enact their therapeutic effects by working on structures within the skin that can convert light to heat energy. These structures get heated up and affect changes to the tissue
Not all human tissue absorbs light as energy. There are only three components of human skin that absorb light as energy, and they are called ‘chromophores.’
The three chromophores in human skin are:
Each of these ‘chromophores’ aabsorbslight at different wavelengths preferentially.
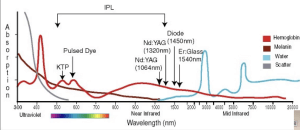
Using this chart, you can see that the bottom line demonstrates wavelengths of laser (measured by units nm) and theleft-handd height of the graph represents how much each component of skin can absorb the light energy.
Scatter is a component of lasers that makes them inefficient and non-useful, so any wavelength that scatters is not used for cosmetic purposes.
The result is the following:
Wavelengths to treat haemoglobin (spider veins aka telangiectasias, or rosacea), would be best to use a 430nm laser, however that wavelength is subject to scatter. The next two best wavelengths are 580nm or somewhere in the 950 to 1050 range.
The most commonly used vascular laser is the Nd: YAG. The name refers to the components of the laser that create the light energy. It is neodymium: Ytrrium Aluminium Garnett.
Spider veins can be effectively treated by a vascular laser, as the pulses of light energy are converted to heat by haemoglobin. The haemoglobin reaches 70 degrees Celsius after a very brief pulse of light, causing the vessel to coagulate. It then gets reabsorbed by the body in the following week.
The main risk of this procedure is the potential heating of the tissue around the targeted blood vessel. Skin that gets overheated can blister. For this reason, the tissue surrounding the targeted vessel is cooled pre and post-treatment using attachments to the laser device
Often you will need two to three treatments with a laser to remove the spider veins. They will come back in new locations eventually, but this usually takes years and you can attend for further laser treatments whenever this happens.